Scheuermann's Disease - A Disease or Not?
Alot of conditions have long
and sometimes scary names. Scheuermann’s disease is one such condition.
It occurs in children and is quite common,
quoted in some studies as occurring in 25% of all children to varying degrees.
Although the condition has an horrific name, it is not a terrible problem.
Scheuermann's disease usually becomes apparent at school with the advent of
some deformity, and it can be accompanied by backache and stiffness, usually
aggravated by sitting. During the onset, the child's posture often changes. The
back curve may become exaggerated and the child who develops the condition is
often told by his parents and teachers not to slouch. The backache can be in
the middle and lower back.
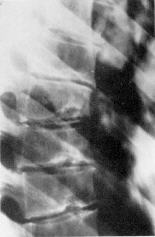
The condition was originally described by
Scheuermann, who stated that the diagnosis was established if there was wedging
of vertebral bodies, in association with other changes, including
intervertebral disc space narrowing, Schmorl's nodes, and deformity. These
changes can occur with or without pain. Small changes in the growing parts of
the vertebrae may be seen. These changes may persist and predispose the lower
thoracic spine to degenerative changes later in life.
Scheuermann's disease usually lasts as a
symptomatic pain producing problem between 6 months and 3 years. It is a
problem in growing adolescent, and once the growth is finished the condition
recovers. The function of the spine and hamstring muscles is usually mildly
affected in the long term, emphasizing the need for rehabilitative exercises.
Treatment
The treatment of
Scheuermann's disease depends upon the severity of pain and the degree of
mechanical changes seen on examination. The pain may become prominent during
the growth phase of the spine. When more severe, relative rest from activity is
necessary. The traditional treatment was rest, especially in large back braces,
however, this treatment was excessive.
The range of treatment is as follows:
![]() Exercises
Exercises
The back can become very stiff during the
active phase of this condition. It is important to attempt to maintain
mobility. The thoracolumbar region, most affected by the condition, moves
particularly in rotation and so stretching in all ranges, especially rotation,
is necessary. Strengthening exercises associated with postural modification is
usually very important and specific instructions are required.
![]() Rest
Rest
The more the condition is accompanied by
pain, back mobility changes, postural deformities and hamstring tightness, the
more that rest will be required. This can mean complete rest from active
contact sports such as football, and rest from activities requiring repetitive
overload, e.g. long distance running, bowling in cricket, gymnastics, ballet
dancing, etc.
![]() Physical Therapy
Physical Therapy
The major role for this therapy in
Scheuermann's disease is to assist in providing an exercise program. Physical
therapy such as mobilisation and manipulation aimed at the stiffest lower
thoracic spine may be tried on 2 - 6 occasions, but the treatment should be
performed with care and only continued if improvement is obvious and
attributable to physical therapy, rather than to exercises and time. Some
Practitioners suggest manipulation to other areas of the spine, eg. the neck or
sacro-iliac joints, will help. It is probable that this form of therapy should
be avoided.
![]() Day to day activities
Day to day activities
General fitness should be maintained.
Swimming is probably the best form of exercise, but may not help with pain
relief. A modified general exercise program will assist with fitness and the
degree of pain and stiffness during and after activity will indicate how much
can be done. Sitting is often the most aggravating activity. It is important to
find a comfortable posture, especially at school. A lumbar roll may help. If
pain is prominent during classes, it may be necessary to stand and do
stretching exercises. A light velcro back brace that does not limit mobility
may help with pain control. Tablets such as aspirin or paracetamol may be useful
during painful times, e.g. during examinations or long periods of study. If the
deformity is accompanied by foot deformity, particularly flat feet, then
orthotic devices may be required.
![]() Later treatment
Later treatment
As this condition is time limiting, there is
no specific treatment if the condition is detected in later life. Sometimes an
adult may present with backache. X-rays may be taken which show old
Scheuermann's disease changes. No specific inference should be drawn from these
x-ray changes, except to say that the effected segments of the spine, usually
the thoracolumbar region, will be stiffer than would normally be expected. As
pain cannot be attributed to degenerative changes, they are irrelevant in the
context of pain origin. If stiffness and/or weakness exists, the treatment may
well include physical therapy and exercises.
Scheuermann's disease is just one of the
many conditions found in the population incidentally. Treatment should address
the signs and symptoms of the presenting condition, and not the incidental
radiological findings.